$130.00
**Please use patient first initial and complete last name**
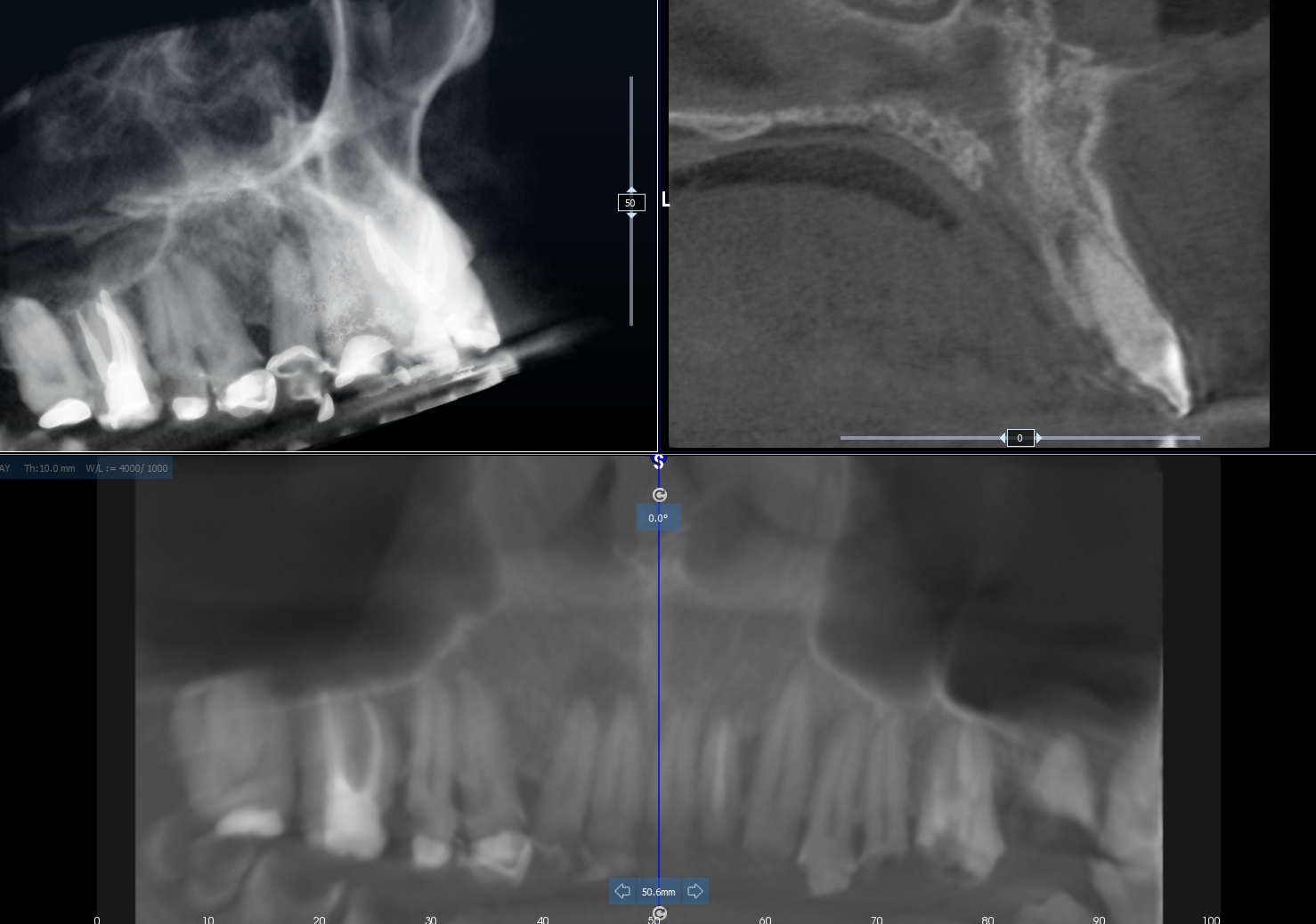
Patient’s medical history, information about the area of interest. (please where applicable provide description, location, signs, symptoms, previous treatment history, working diagnosis, dates of 2D radiographs provided and other pertinent information)